


In this series, “The Miraculous Immune System,” we’ll explore the true power of our immunity, the organs that work tirelessly to protect us. We’ll also provide practical ways to protect these vital gifts from the divine.
Tonsillectomies have long been considered to be relatively minor surgeries, yet recent evidence of associated risks and long-term consequences warrant second thoughts about rushing into surgery.
As the guardians against pathogens, the tonsils are a front line of defense and the first major mucosa-associated immune barrier that foreign microorganisms have to confront to enter the digestive tract.
Tonsil removal, therefore, allows harmful pathogens to enter the digestive tract without being detected, altering intestinal flora by influencing bacterial colonization or invasion of the alimentary tracts, leaving the body vulnerable to serious, potentially life-threatening conditions.
Esophageal cancer is a dangerous type of cancer that more than 80 percent of people don’t survive for more than five years. About 21,560 new cases of esophageal cancer and 16,120 deaths from the disease are projected to occur in the United States in 2023, according to the American Cancer Society.
In a retrospective cohort study published in PLoS One in 2020, doctors evaluated the association between tonsillectomy and esophageal cancer. They looked at 452 patients who had esophageal surgery, including 396 with cancer and 56 with a pre-cancerous condition. The doctors also looked at 1,102 patients who had surgery on their chest but not on their esophagus.
Cases with esophageal cancer or a pre-cancerous condition had a 19.9 percent tonsillectomy history, which is significantly higher than that of control cases (12.7 percent; p-value = 0.0003). This association remained even when accounting for other known risk factors for esophageal cancer, such as obesity, gastroesophageal reflux disease, and smoking.

Esophageal cancer patients had a higher chance of having had a tonsillectomy. (The Epoch Times)The study mentioned that the exact reason behind this connection isn’t known, but one possible explanation is that the removal of tonsils may cause an imbalance in the microbiome of the esophagus, intestines, or both, which can lead to exposure to harmful bacteria and uncontrolled activation of inflammatory pathways, potentially affecting the immune system.
Additional studies have found that the diversity of bacteria in the esophagus differs in people with pre-cancerous lesions and esophageal cancer. These conditions are linked to an increase in harmful bacteria and a decrease in beneficial bacteria. The change in the composition of bacteria may trigger a change in the response pattern of innate immunity, including toll-like receptors and cytokine profiles, leading to inflammation-associated cancer contributors and the development of cancer.
Multiple studies have also shown that reduced levels of secretory antibodies such as immunoglobulin A (IgA) after tonsillectomy. Mucosal IgA is a type of antibody that protects against mucosal pathogens; low IgA levels can contribute to increased proinflammatory status and an increased risk of disease, including cancer.
Because tonsils are the gatekeepers of immunity, the risk of developing esophageal cancer can increase when the tonsils are gone.
Throat cancer and tonsil cancer can occur when there’s an abnormal growth of cells in the middle part of the throat, the oropharynx. More than 90 percent of these cancers are squamous cell carcinomas, which means they start in the thin, flat cells that line the throat.
The number of cases of oropharyngeal carcinoma is increasing at an alarming rate around the world, especially in developed countries, and is affecting younger people and more men. This increase is mostly due to human papillomavirus (HPV), which spreads through sexual contact and is the main cause of oropharyngeal carcinoma.
There are two types of oropharynx cancer: HPV-associated and non-HPV-associated. HPV-associated cancer is caused by a type of virus that spreads through oral sex. This type of cancer is becoming more common, especially in younger people and men. Non-HPV-associated throat cancer is mostly caused by smoking and heavy drinking.
Tonsil cancer is the most common form of oropharyngeal cancer, and even those who’ve had a tonsillectomy still have a chance to develop cancer in the tissue that’s left behind.
A study in Denmark published in Cancer Prevention Research involving 90,755 people with a history of tonsillectomy found that although the procedure reduced the risk of tonsil carcinoma in patients under 60, it was associated with a higher risk of oropharyngeal carcinoma, tonsil, and base of tongue cancers in patients over 60 within a year of the operation.
Chronic inflammatory mediators exert multifaceted effects on the development of cancer. On one hand, in the short term, removing the inflammatory tonsil tissues results in less cancer inflammation and favors carcinogenesis, malignant transformation, tumor growth, invasion, and spread. On the other hand, inflammation can stimulate immune effector mechanisms that might limit tumor growth.
The absence of tonsil tissue may correspond to a loss of the local immune response, and in effect, may create a locally immunosuppressed environment. In the long term, this may result in a higher risk of cancers in close proximity.
Researchers at the University of North Carolina–Chapel Hill School of Medicine found that tonsillectomy of people younger than 13 was associated with a nearly two-fold increased risk of tongue cancer and a large decrease in the risk of tonsil cancer. The same trend still exists when considering other risk factors such as sexual history, smoking status, and age.
The study results were based on an analysis of 1,378 controls, 108 base tongue cancer cases, and 198 tonsil cancer cases.
One possible explanation is that patients with a history of tonsillectomy have lingual tonsillar hypertrophy, because the enlargement of the lingual tonsils has been observed in up to one-third of pediatric patients undergoing adenotonsillectomy.
The overgrowth of the lingual tonsil tissues may result in an increased lymphoid tissue, which can also promote tongue cancer.
A population-based case-control study of women living in western New York from 1986 to 1991 found that a history of tonsillectomy was associated with an increased breast cancer risk among premenopausal but not postmenopausal women.
This long-term risk after a tonsillectomy may be correlated with the immune surveillance role of the tonsils.
A national large-scale study from Sweden found that people who had their tonsils or appendix removed before the age of 20 had a higher risk of acute myocardial infarction, also known as a heart attack.
The study followed more than 80,000 people for an average of 23.5 years, including 54,449 who had appendectomies and 27,284 who had tonsillectomies.
The risk of heart attack was increased by 44 percent and 33 percent, respectively, for those who had a tonsillectomy or an appendectomy before age 20. However, the risk wasn’t increased if the procedure was performed after the age of 20. Males and females had similar risk, and it was highest among those who underwent both procedures.
This may be because atherosclerosis, the underlying cause of heart attacks, is linked to inflammation. The removal of other lymphoid organs, such as the spleen, has been shown to accelerate atherosclerosis. Scientists believe that removing the tonsils or appendix may also affect the body’s protective immunity of blood vessels and decrease the immune system’s ability to fight off external pathogens, thereby increasing the risk of atherosclerosis.
It’s also possible that having these procedures done in childhood increases the risk of autoimmune disorders, such as rheumatoid arthritis, which could also contribute to a higher risk of a heart attack.
Removing tonsils might also induce changes in the normal maturation process of immune function in early life, which may alter subsequent cardiovascular risk.
About 7 to 16 percent of the population in the United States is affected by irritable bowel syndrome (IBS). The disorder has subtypes that are categorized by diarrhea, constipation, or both. IBS can cause stomach and bowel problems such as diarrhea, constipation, bloating, gas, and stomach pain. Aging, stress, and smoking are common risk factors, and IBS is more common among females.
In a 2020 PLoS One study, researchers in Taiwan examined the risk of developing IBS after tonsillectomy by analyzing data from 1,300 tonsillectomy patients and 2,600 matched controls.
The study found that tonsillectomy was associated with a higher risk of developing IBS. The incidence of IBS in tonsillectomy patients increased by 80 percent and was even higher for tonsillectomy patients over 50 years old.
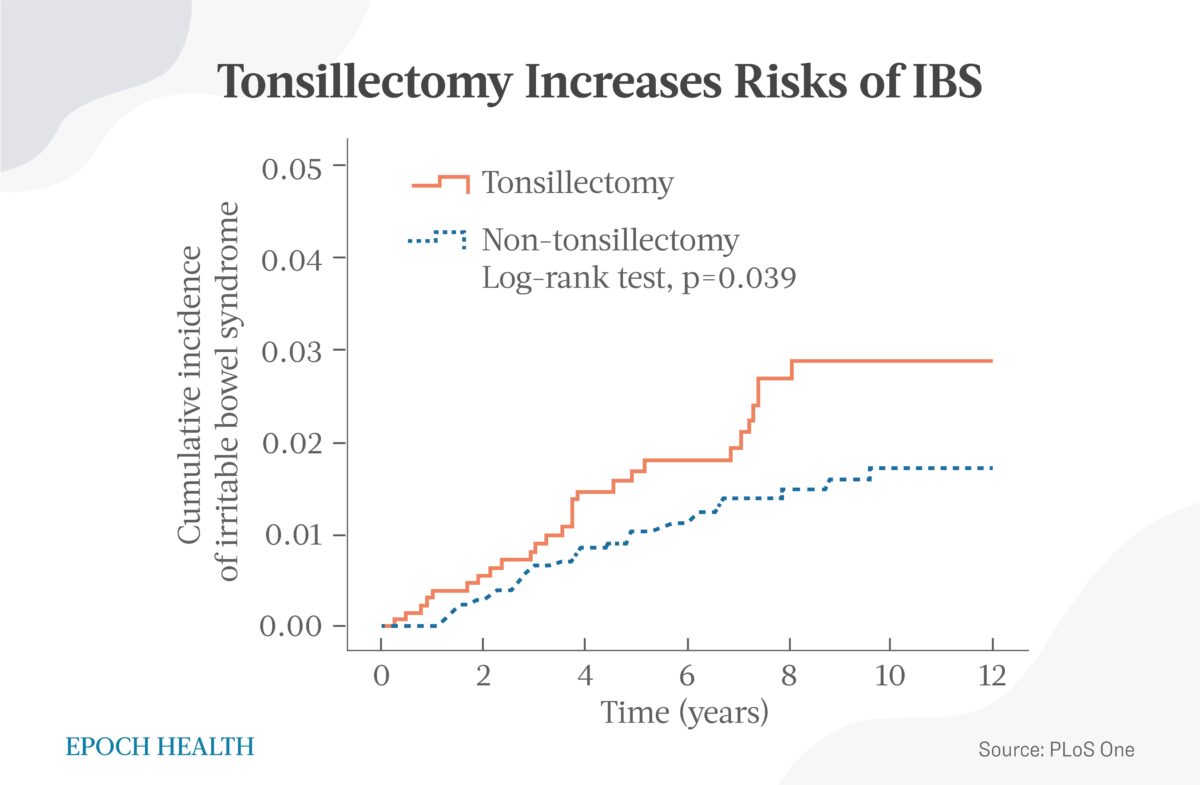
Tonsillectomy increases the risk of irritable bowel syndrome. (The Epoch Times)A reduction in secretory IgA levels after tonsillectomy can last for more than 20 years. Dysbiosis of the intestinal microbiome and a decrease in bacterial diversity is associated with the pathogenesis of IBS.
Tonsils help differentiate between commensal and pathogenic bacteria in the alimentary tract and prevent unnecessary immune responses, and tonsillectomy in older patients may show a higher correlation with IBS development than in younger patients.
Similarly, a meta-analysis of 23 observational studies involving 19,569 patients found an increased risk in the development of Crohn’s disease but no association between tonsillectomy and ulcerative colitis.
Tonsillectomy is a common procedure for treating recurrent tonsillitis and other conditions, but it isn’t always necessary or best for everyone. As with any medical procedure, there are risks and benefits to consider, and it’s important to discuss these with a health care professional to determine the best course of action. Physicians, patients, and families may want to take these findings into consideration when considering a tonsillectomy.
Tonsillectomy is often considered a minor procedure in children, but it comes with risks of complications, such as respiratory problems, nausea, vomiting, pain, and even death. Tonsillectomy has shown short-term benefits such as reduced throat infections and better sleep outcomes.
Long-term risks associated with tonsillectomy include increased risk of infections, respiratory disease, cancers, acute myocardial infarction, and intestinal diseases, some of which are life-threatening. These unexpected long-term effects of tonsillectomy are reminders of the natural healing power and immunity of the human body.
Although there may be a motivation to remove tonsils to quickly resolve symptoms, it may not be easy to repair the body’s divinely endowed natural immunity and could lead to more severe consequences.
Next: The lymphatic system is our “immune network manager” designed to keep internal and external toxins away from our body. However, its true healing power extends beyond that. There are five simple ways to strengthen it.
Rustgi, A. K., & El-Serag, H. B. (2014). Esophageal carcinoma. The New England Journal of Medicine, 371(26), 2499–2509. https://doi.org/10.1056/NEJMra1314530
Yang, L., Lu, X., Nossa, C. W., Francois, F., Peek, R. M., & Pei, Z. (2009). Inflammation and intestinal metaplasia of the distal esophagus are associated with alterations in the microbiome. Gastroenterology, 137(2), 588–597. https://doi.org/10.1053/j.gastro.2009.04.046
Abrams J. A. (2017). The microbiome as a potential biomarker for oesophageal adenocarcinoma. The Lancet. Gastroenterology & hepatology, 2(1), 4–6. https://doi.org/10.1016/S2468-1253(16)30177-7
Baghdadi, J., Chaudhary, N., Pei, Z., & Yang, L. (2014). Microbiome, innate immunity, and esophageal adenocarcinoma. Clinics in laboratory medicine, 34(4), 721–732. https://doi.org/10.1016/j.cll.2014.08.001
O’Riordan, J. M., Abdel-Latif, M. M., Ravi, N., McNamara, D., Byrne, P. J., McDonald, G. S., Keeling, P. W., Kelleher, D., & Reynolds, J. V. (2005). Proinflammatory cytokine and nuclear factor kappa-B expression along the inflammation-metaplasia-dysplasia-adenocarcinoma sequence in the esophagus. The American Journal of Gastroenterology, 100(6), 1257–1264. https://doi.org/10.1111/j.1572-0241.2005.41338.x
Maeda, S., & Omata, M. (2008). Inflammation and cancer: role of nuclear factor-kappaB activation. Cancer science, 99(5), 836–842. https://doi.org/10.1111/j.1349-7006.2008.00763.x
Chaturvedi, A. K., Anderson, W. F., Lortet-Tieulent, J., Curado, M. P., Ferlay, J., Franceschi, S., Rosenberg, P. S., Bray, F., & Gillison, M. L. (2013). Worldwide trends in incidence rates for oral cavity and oropharyngeal cancers. Journal of Clinical Oncology: official journal of the American Society of Clinical Oncology, 31(36), 4550–4559. https://doi.org/10.1200/JCO.2013.50.3870
Jamal Z, Anjum F. Oropharyngeal Squamous Cell Carcinoma. [Updated 2022 Sep 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK563268/
Yamamura, K., Baba, Y., Nakagawa, S., Mima, K., Miyake, K., Nakamura, K., Sawayama, H., Kinoshita, K., Ishimoto, T., Iwatsuki, M., Sakamoto, Y., Yamashita, Y., Yoshida, N., Watanabe, M., & Baba, H. (2016). Human Microbiome Fusobacterium Nucleatum in Esophageal Cancer Tissue Is Associated with Prognosis. Clinical cancer research: an official journal of the American Association for Cancer Research, 22(22), 5574–5581. https://doi.org/10.1158/1078-0432.CCR-16-1786
Fakhry, C., Andersen, K. K., Christensen, J., Agrawal, N., & Eisele, D. W. (2015). The Impact of Tonsillectomy upon the Risk of Oropharyngeal Carcinoma Diagnosis and Prognosis in the Danish Cancer Registry. Cancer prevention research (Philadelphia, Pa.), 8(7), 583–589. https://doi.org/10.1158/1940-6207.CAPR-15-0101
Multhoff, G., Molls, M., & Radons, J. (2012). Chronic inflammation in cancer development. Frontiers in immunology, 2, 98. https://doi.org/10.3389/fimmu.2011.00098
Zevallos, J. P., Mazul, A. L., Rodriguez, N., Weissler, M. C., Brennan, P., Anantharaman, D., Abedi-Ardekani, B., Neil Hayes, D., & Olshan, A. F. (2016). Previous tonsillectomy modifies odds of tonsil and base of tongue cancer. British Journal of Cancer, 114(7), 832–838. https://doi.org/10.1038/bjc.2016.63
Fricke, B. L., Donnelly, L. F., Shott, S. R., Kalra, M., Poe, S. A., Chini, B. A., & Amin, R. S. (2006). Comparison of lingual tonsil size as depicted on MR imaging between children with obstructive sleep apnea despite previous tonsillectomy and adenoidectomy and normal controls. Pediatric radiology, 36(6), 518–523. https://doi.org/10.1007/s00247-006-0149-7
Brasky, T. M., Bonner, M.R., Dorn, J., Marshall, J.R., Vena, J.E., Brasure, J.R., & Freudenheim, J.L. (2009). Tonsillectomy and breast cancer risk in the Western New York Diet Study. Cancer causes & control: CCC, 20(3), 369–374. https://doi.org/10.1007/s10552-008-9251-5
Mishra, D., Singh, S., & Narayan, G. (2016). Role of B Cell Development Marker CD10 in Cancer Progression and Prognosis. Molecular biology international, 2016, 4328697. https://doi.org/10.1155/2016/4328697
Janszky, I., Mukamal, K. J., Dalman, C., Hammar, N., & Ahnve, S. (2011). Childhood appendectomy, tonsillectomy, and risk for premature acute myocardial infarction–a nationwide population-based cohort study. European heart journal, 32(18), 2290–2296. https://doi.org/10.1093/eurheartj/ehr137
Robinette, C. D., & Fraumeni, J. F., Jr (1977). Splenectomy and subsequent mortality in veterans of the 1939-45 war. Lancet (London, England), 2(8029), 127–129. https://doi.org/10.1016/s0140-6736(77)90132-5
Wu, M. C., Ma, K. S., Wang, Y. H., & Wei, J. C. (2020). Impact of tonsillectomy on irritable bowel syndrome: A nationwide population-based cohort study. PloS one, 15(9), e0238242. https://doi.org/10.1371/journal.pone.0238242
Andreu-Ballester, J. C., Pérez-Griera, J., Ballester, F., Colomer-Rubio, E., Ortiz-Tarín, I., & Peñarroja Otero, C. (2007). Secretory immunoglobulin A (sIgA) deficiency in serum of patients with GALTectomy (appendectomy and tonsillectomy). Clinical immunology (Orlando, Fla.), 123(3), 289–297. https://doi.org/10.1016/j.clim.2007.02.004
Wang, L., Alammar, N., Singh, R., Nanavati, J., Song, Y., Chaudhary, R., & Mullin, G. E. (2020). Gut Microbial Dysbiosis in the Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis of Case-Control Studies. Journal of the Academy of Nutrition and Dietetics, 120(4), 565–586. https://doi.org/10.1016/j.jand.2019.05.015
Sun, W., Han, X., Wu, S., & Yang, C. (2016). Tonsillectomy and the risk of inflammatory bowel disease: A systematic review and meta-analysis. Journal of Gastroenterology and Hepatology, 31(6), 1085–1094. https://doi.org/10.1111/jgh.13273
Ford, A. C., Lacy, B. E., & Talley, N. J. (2017). Irritable Bowel Syndrome. The New England Journal of Medicine, 376(26), 2566–2578. https://doi.org/10.1056/NEJMra1607547
Nam, S. Y., Kim, B. C., Ryu, K. H., & Park, B. J. (2010). Prevalence and risk factors of irritable bowel syndrome in healthy screenee undergoing colonoscopy and laboratory tests. Journal of Neurogastroenterology and Motility, 16(1), 47–51. https://doi.org/10.5056/jnm.2010.16.1.47