



The September 9 hearing on vaccine safety led by Sen. Ron Johnson (R-Wis.) exposed what many Americans are now beginning to realize: the medical community has arguably been duped into believing that vaccines are unequivocally safe. The hearing, titled “How the Corruption of Science has Impacted Public Perception and Policies Regarding Vaccines,” was led by Johnson’s Permanent Subcommittee on Investigations. It followed other hearings conducted by Johnson on the subject of COVID-19 pandemic and the COVID-19 mRNA shots.
Three witnesses — physician Dr. Jake Scott, attorney Aaron Siri, and Stanford infectious diseases researcher Dr. Toby Rogers, with Scott defending vaccine research and trials and Siri and Rogers questioning them — offered sharply divergent pictures on the reliability of vaccine research and, by extension, vaccine safety. Both camps cited data, but Siri and Rogers proved to be the more nimble and better-informed interpreters of the evidence. Taken together, their testimony reinforced the growing impression that vaccines have never been subjected to the kind of rigorous study the public assumes.
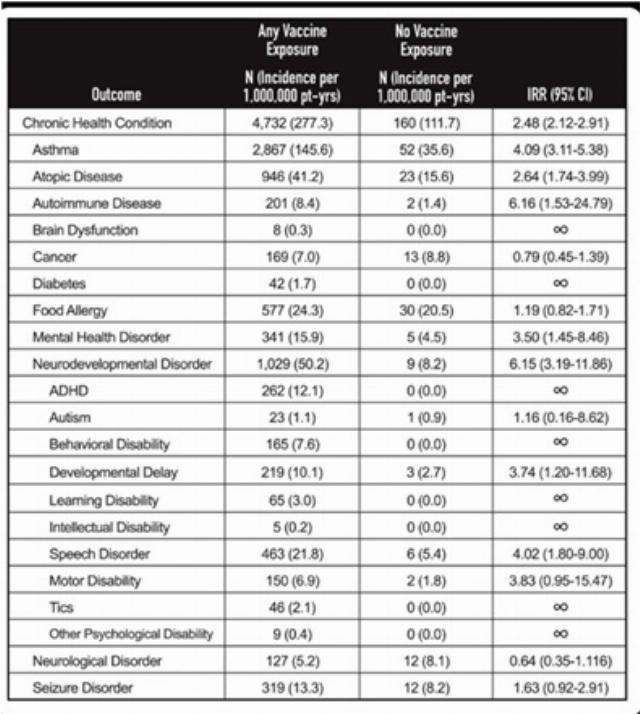
Importantly, the committee put into the public record two irreconcilable records about how vaccine safety should be demonstrated. Siri submitted to the committee an unpublished study conducted inside Henry Ford Health in Detroit. The Ford study contends that real-world comparison is the most meaningful. It studied two cohorts over time, vaccinated vs. unvaccinated children, showing large, repeated signals of vaccine harm in the Ford health system.
The study tracked 18,468 children from birth within the Henry Ford system (1,957 unvaccinated, 16,511 who received at least one vaccine). Using Cox proportional hazard models, the analysis found that vaccination exposure was independently associated with elevated risks across several outcomes: any chronic condition (HR 2.53, 95% CI 2.16–2.96), asthma (HR 4.25, 3.23–5.59), autoimmune disease (HR 4.79, 1.36–16.94), atopic disease (HR 3.03, 2.01–4.57), eczema (HR 1.31, 1.13–1.52), and neurodevelopmental disorder (HR 5.53, 2.91–10.51).
According to the abstract, the 10-year likelihood of remaining free of any chronic condition was 83% among unvaccinated children versus 43% among those vaccinated, as provided below, per Siri’s testimony:
Siri explained that the study provides
a real-world example of how the science around vaccines gets corrupted; how only studies that confirm the beliefs and policies that vaccines are safe get published. Everything else gets shoved in a drawer. This selection bias is dangerous and results in corrupting all the science concerning vaccine safety.
He added that the scientists who conducted the study set out to prove that “childhood vaccines are safe.” However, the researchers “found the opposite” but were afraid to publish it for fear of losing their jobs — a believable sentiment in light of what happened to so many physicians and scientists during the pandemic.
Scott flagged what he believes to be classic biases in vaccinated-vs.-unvaccinated designs: The never-vaccinated children had about half the follow-up time of vaccinated peers; neurodevelopmental diagnoses were counted only after age 2; and never-vaccinated children had substantially fewer health care encounters, reducing opportunities for diagnosis. He added that even amid those imbalances, no association with autism was observed in that dataset.
In addition, Scott asserted, studies like the Ford analysis are inherently confounded by follow-up time and health care utilization, and that when one uses randomized or registry-based methods with strong controls, one doesn’t see broad increases in chronic disease — but one does see rare risks when they exist.
In contrast, Scott submitted a very different thesis, based on the theory that the public record already contains a vast, transparent evidence base. He highlights a global catalogue his team is still compiling — 1,704 randomized controlled trials of vaccines since 1941 involving more than 10.5 million participants, including 661 trials that allegedly used inert (saline or equivalent) placebos, with direct PubMed links.
He also inventoried three main safety platforms — VAERS, Vaccine Safety Datalink (VSD), and PRISM — arguing that they’re sensitive enough to detect harms “as rare as 1 per million doses” and have, in fact, identified true signals that led to warnings and policy changes. If vaccines were driving a broad epidemic of chronic disease, he argues, such systems would have already seen it.
Siri, however, torched the claim that inert substances are used as controls with a level of specificity that was difficult for Scott to contradict.
“That leaves us with three studies,” Siri continued — “three that were claimed to have an inert control that were relied upon to license the routine injected childhood vaccine at this entire list of 661. And these actually helped really highlight the problem we have in terms of assessing safety with regards to the licensure of childhood vaccines.”
Siri elaborated: “One was a trial for the chickenpox (varicella) vaccine that used an injection of neomycin, an antibiotic,” as its “inert” substance. Siri then stated the second was a Gardasil 4 trial with “thousands and thousands of girls and women in the control group. Almost all of them got an aluminum adjuvant injection. A few hundred of them were labeled inert ... but they got everything in the Bible ... including histidine 80, sodium borate, and yeast protein.” The third was a Gardasil 9 trial, in which about 100 girls and women out of thousands did receive a saline injection, but “only after they got the first three doses of Gardasil 4.”
Rogers’s testimony focused primarily on the rise in autism and the inadequacy of current research. As a doctoral student in political economy at the University of Sydney, Rogers meticulously reviewed the CDC’s cited causes of autism and found each explanation lacking:
Scott, a Stanford-affiliated infectious disease specialist, seemed unprepared for Siri’s rigorous, line-by-line dissection of the data being presented on both sides of the argument. Some read Scott as arrogant. However, that perception may be more reflective of an ecosystem that produces the dogmatic information gaps many clinicians face. Those gaps, reinforced by pharmaceutical influence and federal agency orthodoxy, create persistent cognitive dissonance when confronted with data that challenge prevailing assumptions. Scott struggled to reconcile the two.
Sadly, Scott’s response mirrored that of many conventional physicians when confronted with contradictory, inconvenient evidence. Siri’s findings diverged sharply from the narrative that has dominated the vaccine industry for decades. It seemed as if this was the first time Scott had encountered some of the information Siri was presenting.
Scott’s responses felt simultaneously pathetic and tragic. He appeared to genuinely care about his patients, but his sincerity was undermined by a professional framework shaped by decades of selective research and institutional messaging. To his credit, when invited by Johnson, Scott expressed willingness to return and debate COVID-19-related issues in greater detail — something most like-minded physicians are reluctant to do.

Image: Triggermouse via Pixabay, Pixabay License.